When our most vulnerable citizens aren’t dying from a lack of healthcare, they’re dying from DIY pain relief furnished by opioid manufacturers. And our governments — all 50+ of them — for the most part appear flummoxed by the scale of the emergency.
How is our country doing with the opioid epidemic? Are we looking at a turning tide, or is a lack of action still digging a deeper hole for future generations to climb out of?
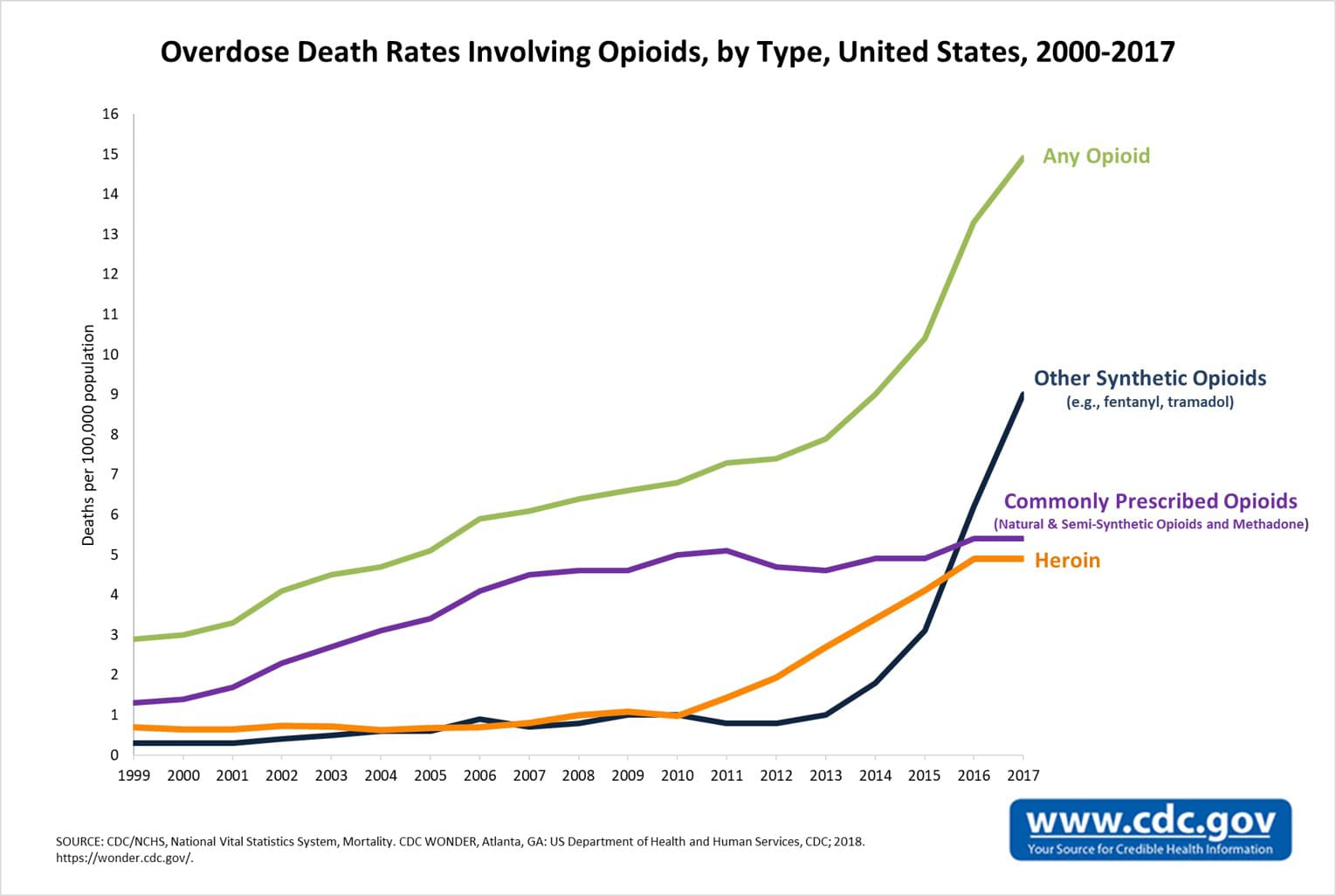
Opioid Use and Overdose: State of the Union
According to numbers furnished by the CDC in March 2018, 115 Americans die every day after overdosing from opioid-based pain relievers, heroin, fentanyl and other drugs. All told, opioids represent 40 percent — and climbing — of our nation’s overdose deaths over the last few years.
The crisis represents an annual burden of $78.5 billion on the public coffers, which represents the sky-high cost of lost productivity at work, addiction treatment services, criminal justice proceedings and — of course — general healthcare.
In other words, this is both a moral and economic disaster — and just as we’re “punting” the “inconvenience” of climate change down the line for future generations to deal with, so too are we “punting” on opioids. Alongside our rafts of preventable deaths, we’re also seeing those who enter this world already in withdrawal thanks to their mothers’ opioid habits.
This is a catastrophe — and a public health emergency unlike almost anything else we’re facing right now.
What’s Our Congress Doing About It?
It’s obvious that Congress’ failures are our failures first. They frequently do nothing even when we demand action — but they definitely do nothing when we don’t.
In April 2018, a bipartisan health committee based in the Senate approved the Opioid Crisis Response Act of 2018. The next step is holding hearings for six months and accumulating reports on the best path forward. This would seem like a strong message that the Senate, at least, considers this a real threat and is open to pursuing action to help bring it to heel.
So, what does the Act propose?
Experts are worried it would “tinker” at the fringes instead of attacking the problem head-on. The Act seeks to empower the Department of Health and Human Services to target the states with the highest rates of opioid-related mortality — including Native American tribes — with newly redirected federal funds specifically for fighting this epidemic via consumer education, healthcare and other measures. A grant program would let at-risk and hard-hit states establish Comprehensive Opioid Recovery Centers using a newly authorized grant program.
The Act also contains new guidelines and requirements, such as a week-long allotment of medication instead of a larger quantity that could encourage misuse.
America’s House of Representatives is pursuing a similar agenda of its own. Together, the two chambers of our bicameral legislature have gone about addressing this problem differently than the executive branch, which labeled the situation a “health emergency.” Other than recommending stricter criminal justice measures for everybody involved — except pharma CEOs — neither the president nor much of his administration seems troubled overmuch by the progress of the crisis or our lack of same.
The medical community praises the Act for spending in the right places but worries its measures still aren’t enough. Baltimore’s Health Commissioner, Leana Wen, said: “Many of these policies seem to be tinkering around the edges … [we need] sustained, specific funding.”
The problem is a simple and exasperating one. None of the measures proposed by the Act would actually increase our healthcare spending — it’s more a “restructuring” of existing funding sources, with the details left for future appropriations negotiations in Congress to hammer out. But the worst part is that the “restructured” funding sources only address opioid victims who have actively sought treatment for their situation.
How many Americans does that represent? According to the office of the Surgeon General, just 10 percent of those of us who struggle with substance abuse seek treatment.
Judging by the damning fine print, Congress has failed on every front to confront this moral and economic disaster meaningfully, even as it spirals further out of control. They have failed to allocate a sum of money that would make a significant difference, they have failed to recognize that most of our opioid victims don’t actually seek treatment and they have failed yet again by conveniently forgetting that even if these people were inclined to seek medical treatment, our broken healthcare system is wholly incapable of treating them in a cost-effective way.
Republicans and Democrats alike are not champions of public health nor of a reasonable public healthcare system. They don’t talk about healthcare as a human right. Instead, they talk about universal “access” to healthcare — and then do nearly nothing at all to make sure such a thing actually exists. Now that we need it more than ever, their tone-deafness and lack of backbone are more conspicuous today than at any point in our collective memory of American democracy.
The Battle Moves to the States
The presidency of Donald Trump is not a rebuke of centralized authority — it’s a rebuke of centralized authority that doesn’t care about human life. Because of the leadership black hole Washington has become, the battle for healthcare dignity — and an end to the opioid epidemic — has moved to the states.
America is a patchwork of governments, some of which are choosing to do more than others when it comes to practical ways to reduce opioid deaths. Access to buprenorphine — the “gold standard” for treating opioid addiction — has become a bellwether for a state’s willingness and preparedness to help solve this problem. This litmus test reveals which states are working toward a solution and which are not.
New Hampshire, Ohio and West Virginia, for example, all have high rates of opioid overdoses and yet have not increased funding for or access to buprenorphine or other treatment techniques.
Are health experts being kept out of the loop? Some folks say they are. Most physicians and authorities on the subject maintain even a federal investment of $100 billion over the next half-decade wouldn’t be enough to make a dent in this problem. But they also say our punitive-based measures, such as those the Trump administration is pursuing, are precisely the wrong way to go about it.
States like Vermont are showing we need to treat our way out of this — including by taking public health seriously. The state’s determination that addiction is a public health issue has resulted in their having one of the relatively lowest opioid death rates in the country.
Common sense and mathematics are on their side. We find time and time again that the states that make investments in the health of their citizens enjoy greater happiness and productivity — plus, they free themselves from the crippling financial burden of leaving health crises unaddressed and therefore have more revenue to tackle their other problems, such as our dangerously crumbling infrastructure.
From a morally compassionate and “fiscally conservative” standpoint, taking this epidemic seriously is the only course open to a country that believes so hard in its own exceptionalism.







{kind=link}
@kolohe’s comment on the Clancy thread was just too perfect to leave there:
Report
Except instead of the big bad being Medellin, it’s Eli Lily.Report
I’ve read that, while big cities are taking steps to reduce mass incarceration, the opioid crisis is driving rural people into prisons in numbers that offset urban declines. Whether that will wake up a larger constituency to criminal justice reform is yet to be seen.
I’m not sure that racial solidarity will make white people see people convicted of crimes as worthy of consideration/sympathy in the same way as the black community. After all, there is no other “oppressor” to blame if people aren’t getting mad at Big pharma and still identify with cops. White identity politics is on the rise, but old habits die hard.Report
I know that conspiratorial thinking is not likely to be particularly fruitful but… damn. I can’t help but notice that opioids are patentable and responsible for billions of dollars in profits and the corporations that make them are willing to spend millions on lobbying.
Studies seem to show that legal marijuana lowers opioid use. So, of course, opioid manufacturers are involved with lobbying against legalized marijuana. Gillibrand, at least, has noticed and has called big pharma out… but, man.
I’m trying to avoid conspiratorial thinking… but the argument that the system has been captured is one that I can’t escape. Congress is complicit, the FDA is complicit, the Attorney General is complicit. The people who get hurt don’t matter beyond their ability to pay for more of the product.Report
I don’t think you need conspiratorial thinking in this case – the pharma companies are doing what is individually rational and profitable for them. Collusion / conspiracy is unnecessary to explain the observed behaviour.Report
Where Are We at with the Opioid Epidemic?
Oh, the Opioid Epidemic is going quite well, thanks for asking.Report
Fun side effect of all this is, when you go to the doctor with pain-involved health problems that are not glaringly obvious, at least some of them now immediately dismiss you as a drug seeker (in addition to a hypochondriac and a hysteric, if you’re a woman). This in turn leads to more medical expenditures than would otherwise be required as patients have to go back again and again saying “no, seriously, something is actually wrong here” and often ending up with delayed treatments that cost more money than they should have if you would have been if simply taken seriously to begin with.Report
Argh, that must be really frustrating. I wonder if it would make it better or worse if a person went in with “I hope to get the root cause of my pain addressed, not its symptom suppressed. I do not want opioids and if you prescribe them I will tear the prescription and leave it in the wastebasket in your office.”
I start getting dependent on opioids pretty quickly, to the point where I’d be a bit nervous of taking them even if it were medically indicated.Report
Yes, it’s been pretty irritating. It took 2 years to get in to see a specialist or even to get anything but the most basic of tests, because the immediate assumption seemed to be that unless one is visibly dying, they are at the doctor for some nefarious purpose.
I wish I’d thought of the “I’m not here for drugs” angle to begin with but doctors seem all too eager to assume “this person is here for attention” too. It’s a catch 22 because doctors seem to on the one hand think “if something is really wrong, they’ll come back later” but at the same time “this person keeps coming back, they are obviously lonely/bored/mentally ill.”Report
The 1960’s called. They want their drug debate back.Report